Translate this page into:
Kernohan–Woltman phenomenon: A false localizing sign
2 Department of Cardiac Anaesthesia, Indira Gandhi Medical College, Shimla, Himachal Pradesh, India
Corresponding Author:
Sabina Bhoil
Department of Cardiac Anaesthesia, Indira Gandhi Medical College, Shimla, Himachal Pradesh
India
sabinabhoil@gmail.com
| How to cite this article: Bhoil R, Ahluwalia AK, Surya M, Bhoil S. Kernohan–Woltman phenomenon: A false localizing sign. Natl Med J India 2021;34:56 |
Kernohan–Woltman phenomenon (Kernohan notch), a false localizing sign, is an exception to the general rules of neurological localization, which involves a deficit on the ipsilateral side of the lesion. Initially described with neoplasms, it is commonly seen in the setting of a head injury, associated with haematomas, intracranial space-occupying lesions and spontaneous bleeding of vascular malformations.[1],[2]
A 65-year-old man presented with increasing memory loss, altered personality and decreased concentration for 4 months. He gave history of fall from bed 5 days ago. On presentation, there was decreased cognition, horizontal nystagmus, left hemiparesis and left hyper-reflexia. Non-contrast head computed tomography [Figure - 1]a and [Figure - 1]b done to rule out a right-hemispheric lesion, revealed bilateral subdural haematomas, which were disproportionately more on the left side. The collection was predominantly hypodense on the left side with multiple hyperdense contents within (acute-on-chronic) and hyperdense (acute) on the right side. There was a shift of the interhemispheric fissure to the right and compression of the left lateral ventricle. In addition, the right cerebral peduncle was deformed with obliteration of the right crural cistern.
![[Figure - 1]](#fig_NatlMedJIndia_2021_34_1_56_323452_f1.jpg){kind=link}
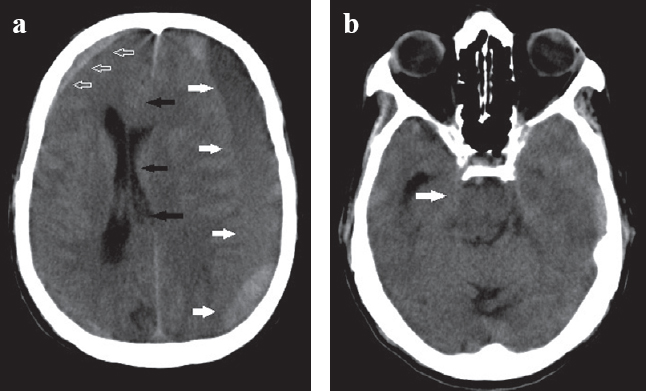 |
| Figure 1: Axial non-contrast computed tomography images of the head showing (a) an extensive left hemispheric acute-on-chronic subdural haematoma (solid white arrows), causing a 1.4 cm midline shift to the right side and compression of the left lateral ventricle (black arrows). A small subdural haematoma (empty white arrows) is also seen on the right side and (b) a left uncal herniation with deformation of right cerebral peduncles and obliteration of the right crural cistern (solid white arrow) |
Kernohan–Woltman phenomenon is an ipsilateral motor weakness caused by compression of the contralateral cerebral peduncle,[1] due to the unyielding nature of tough tentorial attachments leading to a rise in intracranial pressure.[2] Acute uncal herniation causes displacement of the cerebral peduncles on to the tentorium [Figure - 2], and thus injury to this portion of the brain that is traversed by the corticospinal tracts.[2]
![[Figure - 2]](#fig_NatlMedJIndia_2021_34_1_56_323452_f2.jpg){kind=link}
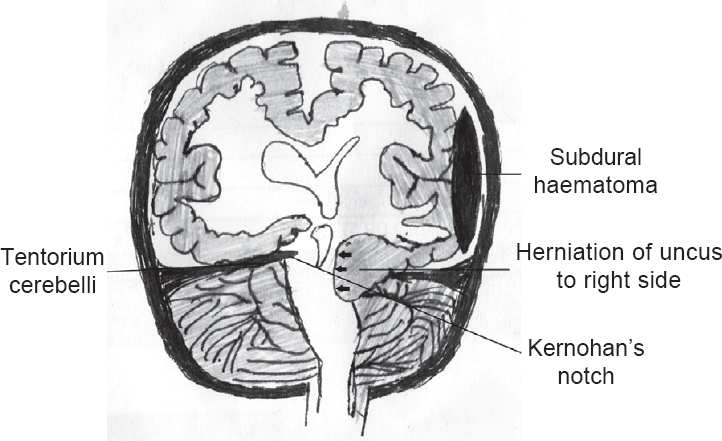 |
| Figure 2: Schematic diagram of uncal herniation (arrows) causing compression of contralateral cerebral peduncle against the tentorium cerebelli |
This sign, though often seen on CT scans, is better visualized on MRI, especially where CT findings may confuse the clinical condition.[1],[2] It is important to recognize this phenomenon, especially in the setting of trauma, when evaluating for laterality of signs and planning emergency management based on clinical and imaging findings.
Conflicts of interest. None declared
| 1. | Zhang CH, DeSouza RM, Kho JS, Vundavalli S, Critchley G. Kernohan–Woltman notch phenomenon: A review article. Br J Neurosurg 2017;31: 159–66. [Google Scholar] |
| 2. | Velasquez JL, Sanz ER, Lasaosa SS, del Val JL. Kernohan’s notch. Pract Neurol 2015;15:221. [Google Scholar] |
Fulltext Views
3,406
PDF downloads
996



