Translate this page into:
The need to focus on medical education in rural districts of India
2 Department of Academics, Public Health Foundation India, New Delhi, India
3 Department of Epidemiology, National Institute for Research in Environmental Health, Bhopal, Madhya Pradesh, India
Corresponding Author:
Kishor Parashramji Brahmapurkar
Department of Community Medicine, L.B.R.K.M. Government Medical College, Jagdalpur, Bastar 494001, Chhattisgarh
India
dr.kishorl710@rediffmail.com
| How to cite this article: Brahmapurkar KP, Zodpey SP, Sabde YD, Brahmapurkar VK. The need to focus on medical education in rural districts of India. Natl Med J India 2018;31:164-168 |
Abstract
Background. Globally, India has the highest number of medical colleges followed by Brazil and China. The density of physicians in rural India was 3 per 10 000 population against 13 per 10 000 in urban areas. Worldwide, studies show that medical schools play an important role in overcoming the shortage of physicians locally. Hence, we studied the distribution of medical colleges in India and reviewed the shortage of established and new medical colleges in rural districts with the year 2000 as baseline.Methods. We used the database of the Medical Council of India as on 27 April 2017; and Census 2011 data, based on the percentage of rural/urban population, for the classification of districts (rural/urban). All the 640 districts were included with 1210.9 million population.
Results. Of the 480 rural districts in India, only 132 (27.5%) had a medical college. Jharkhand, Jammu and Kashmir and Arunachal Pradesh had no medical colleges in rural districts. Madhya Pradesh, Uttar Pradesh, Bihar, Assam, Punjab, Uttarakhand, Haryana and Rajasthan had <30% of rural districts with a medical college. Of the 286 new medical colleges established since 2000 in India, 130 (45.5%) were in rural districts with uneven distribution with lower percentage of new medical colleges in states with predominance of rural population.
Conclusion. There is an overall shortage of medical colleges in rural districts of India. Paradoxically, the trend of uneven rural–urban distribution continues among the newly opened medical colleges as well.
Introduction
Globally, India has the highest number of medical colleges followed by Brazil and China.[1] Even though noteworthy advances have been made in the number of medical training institutions,
India still has a shortage of physicians.[2] The current estimated physician-to-population ratio in India is 1:1700, against a target of 1:1000.[2]
Most doctors (74%) work in urban areas.[3] There are 0.2 beds/ 1000 population in rural areas as compared to 1.1 beds/1000 population in urban areas.[3] There is a shortage of doctors in government health centres in rural areas as compared to urban areas with the density of physicians in rural India at 3 per 10 000 population against 13 per 10 000 in urban areas.[3],[4] We assessed the number of rural medical colleges in India where two-thirds (68%) of the population resides.[5]
Why the need to focus on rural medical education?
The location of medical colleges in rural districts with public ownership is among the variables strongly associated with a tendency to produce rural graduates.[6] Wang found that rural medical schools play an important role in overcoming the shortage of physicians in rural communities.[7]
There is an important role played by government financial support targeted at rural medical education proposals to meet the physician recruitment needs of rural areas.[8] Longombe showed the importance of medical schools in rural areas by observing that 97.7% of graduates from medical schools in rural areas were employed in the rural districts where they were trained.[9] Longombe also found that only 40% of graduates from medical schools in urban areas were employed in the districts where they trained, with 23.7% working in a rural area. This supported the policy of establishing medical schools in rural areas.[9]
Medical schools provide the population living in its vicinity greater access to physicians and specialized care beyond levels that might be available in the routine health system.[10] Medical schools also generate employment opportunities for the local population.[11] Therefore, medical schools have the ability to influence the local healthcare system and the health of the local population.[11]
Training rural health workers in a rural location is likely to enhance recruitment and retention of skilled healthcare providers in the rural areas, and possibly help in limiting the role of quacks in healthcare issues.[12]
Also, WHO had defined social accountability of medical schools as ‘the obligation to direct their education, research and service activities towards addressing the priority health concerns of the community, region and the nation that they have a mandate to serve.‘[13]
Using various methodologies, studies have documented the uneven distribution of medical colleges across India.[14],[15],[16],[17],[18] However, an analysis of medical colleges in India based on the percentage of rural/urban population has not been done. Hence, we studied the distribution of medical colleges in India based on the percentage of rural/urban population of districts. We also reviewed the shortage of medical colleges in rural districts in India with 2000 as the baseline year.
Methods
We used the Medical Council of India (MCI) database as on 27 April 2017.[19] A list of medical colleges for a state was obtained from the website of the MCI and from the Ministry of Health and Family Welfare about autonomous institutes such as the All India Institute of Medical Sciences, Jawaharlal Institute of Postgraduate Medical Education and Research.[19],[20] Population of the states and districts, and percentage of urban/rural population in districts was taken from Census 2011.[5] All the 640 districts of India were included for the study with a total population of 1210.9 million.
Based on the population and number of medical colleges in the states, the number of medical colleges per million population was calculated for states. Districts were identified with the presence of medical colleges and their year of establishment with focus on new medical colleges started after the year 2000.[19]
Classification of all the 640 districts of India based on rural population >70% and urban population >30% was done with the help of district-level factsheets of states of the National Family Health Survey· 2015–16.[21]
Definition of medical college
As per the MCI, a medical college is an academic institute that offers an MBBS course of five-and-a-half years, including 1-year compulsory rotating internship.[2]
Operational definitions of rural districts and shortage of medical colleges
Rural districts were defined as districts with rural population >70% and non-rural/urban districts were defined as districts with urban population >30%. Shortage of medical colleges in a state was defined as >70% of rural districts that did not have a medical college.
Statistical analysis
Data entry was done in Excel, and percentages and ratios were calculated.
Ethics
We used publicly available databases available on the websites of the MCI, Ministry of Health and Family Welfare and Census 2011 data. No ethical approval was sought.
Results
Of the 640 districts, 480 (75%) were rural districts. There were 467 medical colleges but only 132 (27.5%) rural districts had a medical college.
State-wise distribution of medical colleges in rural districts
Only three states, i.e. Andhra Pradesh, Kerala and Telangana, had more than one medical college per rural district [Table - 1]. For non-rural districts, the ratio was more than or equal to one in all states except Jharkhand, Arunachal Pradesh and Haryana. None of the rural districts in Jharkhand, Jammu and Kashmir and Arunachal Pradesh had a medical college. Madhya Pradesh, Uttar Pradesh, Bihar, Assam, Punjab, Uttarakhand, Haryana and Rajasthan had <30% of rural districts with medical colleges as compared to Andhra Pradesh and Telangana with 100% of rural districts with medical colleges. We found that medical colleges tend to cluster in certain metropolitan cities, for example, Bengaluru, Chennai and Kolkata (from Karnataka, Tamil Nadu and West Bengal, respectively) had 12, 10 and 8 medical colleges, respectively. The same was the case in Maharashtra, where Mumbai alone had 9 medical colleges. Two urban districts in Madhya Pradesh, Bhopal and Indore had 11 of the 19 medical colleges in the same state.
![[Table - 1]](#tbl_NatlMedJIndia_2018_31_3_164_255761_t2.jpg){kind=link}
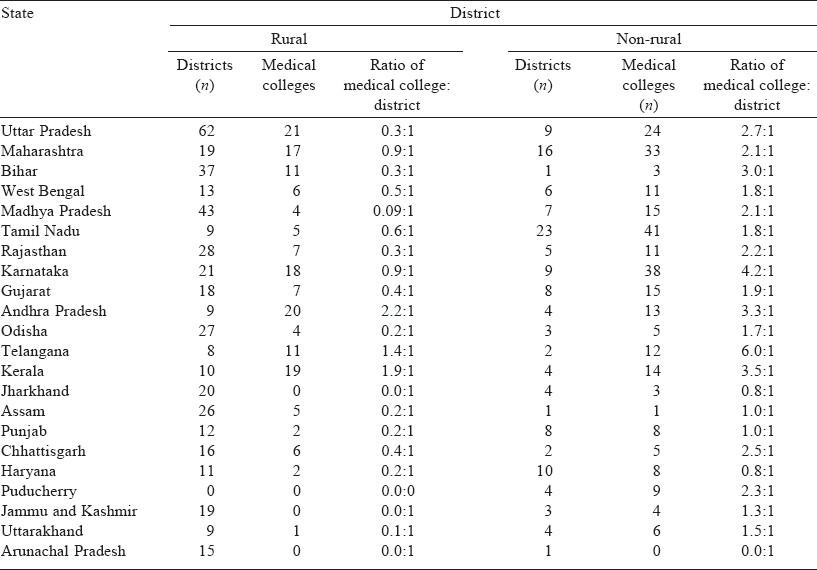
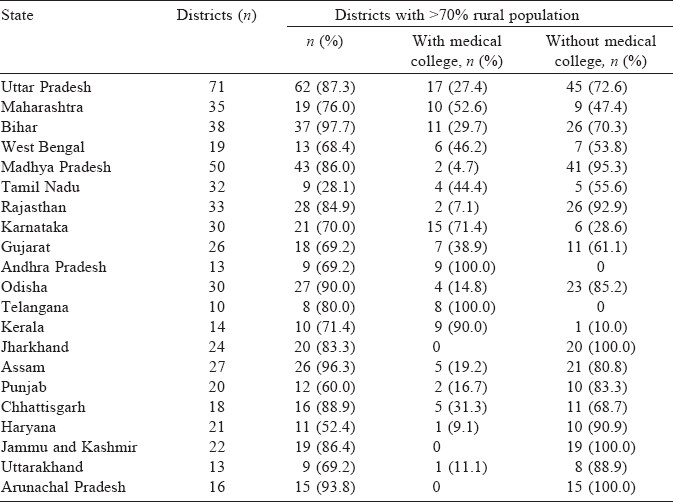
Only 4 (9.3%) rural districts of Madhya Pradesh had medical colleges. In addition, 3 (10.7%) rural districts of Rajasthan had medical colleges and the most populated state Uttar Pradesh with a population of 199.8 million and 62 (87.3%) rural districts had only 21 (33. 9%) rural districts with medical colleges as compared to 100% in Andhra Pradesh and Telangana, respectively [Table - 2], [Figure - 1]. Kerala with 90% of rural districts having medical colleges also had the highest number of medical colleges (0.99) per million population compared to Jharkhand with the lowest number of medical colleges (0.09) per million population.
![[Table - 2]](#tbl_NatlMedJIndia_2018_31_3_164_255761_t3.jpg){kind=link}
![[Figure - 1]](#fig_NatlMedJIndia_2018_31_3_164_255761_f1.jpg){kind=link}
 |
| Figure 1: Number of medical colleges per million population in different states |
New medical colleges established since the year 2000
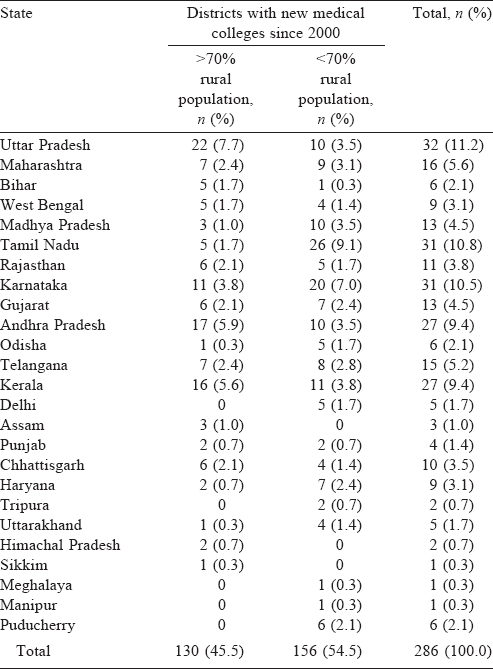
Of the 286 new medical colleges established since 2000 in India, 130 (45.5%) were in rural districts [Table - 3]. Uttar Pradesh which had the highest number of rural districts (62) had 22 new medical colleges established as compared to Kerala with 9 rural districts which had 16 new medical colleges in rural districts. No new medical college was established in Jharkhand which had 20 rural districts. Odisha had only 1 (0.3%) new medical college established in a rural district compared with 5 in non-rural districts (1.7%).
![[Table - 3]](#tbl_NatlMedJIndia_2018_31_3_164_255761_t4.jpg){kind=link}
Discussion
We found an overall shortage of medical colleges in rural districts of Uttar Pradesh, Bihar, Madhya Pradesh, Rajasthan, Odisha, Jharkhand, Assam, Uttarakhand, Haryana, Punjab, Jammu and Kashmir and Arunachal Pradesh as compared to Andhra Pradesh, Telangana, Kerala, Karnataka and Maharashtra. Boulet et al. had mentioned that medical schools were not scattered uniformly at the global level, with 16 nations of Africa not having a single medical school as compared to Belize with a population of 0.27 million having 6 medical schools.[22]
The number of medical colleges per million population was 0.09 in Jharkhand, 0.19 in West Bengal and Assam as compared to 0.99 for Kerala. At the national level, the number of medical colleges per million population was 0.38—Puducherry had the highest, 7.21 medical colleges per million population.[5],[19]
One reason for fewer medical colleges in rural districts could be that people in urban districts were richer and had better paying capacity. The details of pro-rich distribution of medical colleges have been discussed by Sabde et al.[16] and Ananthakrishnan.[23] It has been documented that medical education in a rural location does increase the number of medical graduates who will work in a rural place.[12],[24],[25]
Northern Ontario School of Medicine and Zamboanga School of Medicine are examples of medical schools in rural areas as part of social accountability mandate and these medical schools had shown their impact: more than 67.5% graduates of the medical school were working in rural areas and there was a decline of 86.7% in infant mortality rate over an 8-year period (1995- 2003).[12]
To study the trend in opening of new medical colleges, we studied the rural–urban distribution of medical colleges opened after 2000. We were encouraged that 45.5% of new medical colleges were in rural districts.
However, there were discrepancies in the distribution of new medical colleges in different states. Kerala and Andhra Pradesh with 10 and 9 rural districts had 16 and 17 new medical colleges, respectively, in rural districts (i.e. more than 1 medical college per district). While Jharkhand which had 20 rural districts with no medical college had no new medical college since the year 2000. Hazarika has already documented the inequalities in the availability of health workers in India.[14] As per MCI regulations, for the establishment of new medical college, point number 8 of ‘Essentiality Certificate’ required had mentioned, ‘How the establishment of the college would resolve the problem of deficiencies of qualified medical personnel in the state and improve the availability of such medical manpower in the state?' and all other points to be followed by the MCI stringently before giving no objection certificate to open a new medical college.[23],[26]
Now, as per the proposed National Medical Commission Bill, 2016, the permission for establishment of a fresh medical college will be given by the Medical Assessment and Rating Board (MARB). The proposed MARB should also look in to the shortage of medical colleges in rural districts of India.[26]
One positive move mentioned in the National Medical Commission Bill, 2016, is that the criteria for establishment of a new medical college will be relaxed for underserved areas.[27]
Many MBBS graduates from rural areas are unlikely to serve in their own rural areas after graduation.[23] There was a proposal of 50% reservation of seats for postgraduate (PG) courses in government colleges for those who have provided services for at least 3 years in public healthcare institutions in remote and difficult areas.[28] The proposal, part of the draft Indian Medical Council (Amendment) Bill, 2016, also proposes that such applicants should be required to serve for another 3 years in remote areas after acquiring the PG degree.[28] Quota can be started to get admission to MBBS course for candidates who belong to rural community and ensuring their return with bond to serve in rural and remote areas. This may help in solving the issue of shortage of doctors in rural areas.
We did not study the complex issue of shortfall of health workforce in the concerned states.
Conclusion
There is a shortage of medical colleges in rural districts of India. The shortage is more in certain states such as Jharkhand, Jammu and Kashmir and Arunachal Pradesh (which had no medical college in rural districts).
Since the year 2000, there is a trend of opening new medical colleges in rural districts. However, this trend is confined to the states which already had a number of rural medical colleges. To rectify this paradoxical situation, the MCI should follow regulations related to ‘Establishment of New Medical College’ more stringently.
Conflicts of interest. None declared
| 1. | World Directory of Medical Schools. Available at www.search.wdoms.org (accessed on 27 Apr 2017). [Google Scholar] |
| 2. | Medical Council of India, Vision 2015. Available at www.mciindia.org/tools/ announcement/MCI_booklet.pdf [Google Scholar] |
| 3. | Kishore J. National rural health mission. In: J. Kishore ‘s National Health Programs in India. 11th ed. New Delhi:Century Publications; 2014:99-100. [Google Scholar] |
| 4. | Rao KD, Bhatnagar A, Berman P. So many, yet few: Human resources for health in India. Hum Resour Health 2012;10:19. [Google Scholar] |
| 5. | Census 2011, States; 2011. Available at www.census2011.co.in/states.php (accessed on 3 Jun 2016). [Google Scholar] |
| 6. | Rosenblatt RA, Whitcomb ME, Cullen TJ, Lishner DM, Hart LG. Which medical schools produce rural physicians? JAMA 1992;268:1559-65. [Google Scholar] |
| 7. | Wang L. A comparison of metropolitan and rural medical schools in China: Which schools provide rural physicians? Aust J Rural Health 2002;10:94-8. [Google Scholar] |
| 8. | Tesson G, Curran VR, Strasser RP, Pong RW. Adapting medical education to meet the physician recruitment needs of rural and remote regions in Canada, the US and Australia. In: Rotem A, Perfilieva G, Dal Poz MR, Doan BD (eds). National health workforce assessment of the past and agenda for the future. Paris :Centre de Sociologie et de Démographie Médicales; 2006. [Google Scholar] |
| 9. | Longombe AO. Medical schools in rural areas—necessity or aberration? Rural Remote Health 2009;9:1131. [Google Scholar] |
| 10. | Ko M, Heslin KC, Edelstein RA, Grumbach K. The role of medical education in reducing health care disparities: The first ten years of the UCLA/Drew Medical Education Program. J Gen Intern Med 2007;22:625-31. [Google Scholar] |
| 11. | Shankar P. Privatization of medical education in Nepal and South Asia: An important area for future research. Webmedcentral Med Educ 2011;2(11):WMC002471 doi: 10.9754/journal.wmc.2011.002471. Available at www.webmedcentral.com/ article_view/2471 (accessed on 27 Apr 2017). [Google Scholar] |
| 12. | Strasser R, Neusy AJ. Context counts: Training health workers in and for rural and remote areas. Bull World Health Organ 2010;88:777-82. [Google Scholar] |
| 13. | Boelen C, Heck J. Defining and measuring the social accountability of medical schools. Geneva:WHO; 1999. Available at www.apps.who.int/iris/bitstream/10665/ 59441/1/WHO_HRH_95.7.pdf (accessed on 2 Jul 2016). [Google Scholar] |
| 14. | Hazarika I. Health workforce in India: Assessment of availability, production and distribution. WHO South East Asia J Public Health 2013;2:106-12. Available at www.searo.who.int/publications/journals/seajph/seajphv2n2_p106.pdf (accessed on 16 Mar 2016). [Google Scholar] |
| 15. | Rao M, Rao KD, Kumar AK, Chatterjee M, Sundararaman T. Human resources for health in India. Lancet 2011;377:587-98. [Google Scholar] |
| 16. | Sabde Y, Diwan V, De Costa A, Mahadik VK. Mapping the rapid expansion of India’s medical education sector: Planning for the future. BBMCMedEduc 2014; 14:266. [Google Scholar] |
| 17. | Mahal A, Mohanan M. Growth of private medical education in India. Med Educ 2006;40:1009-11. [Google Scholar] |
| 18. | Mahal A, Mohanan M. Medical education in India, implications for quality and access to care. J Educ Plann Adm 2006;20:473-84. [Google Scholar] |
| 19. | Medical Council of India, Information Desk. Available at www.mciindia.org/ InformationDesk/CollegesCoursesSearch.aspx (accessed on 11 Jul 2016). [Google Scholar] |
| 20. | Ministry of Health and Family Welfare, Autonomous bodies. Available at www.mohfw.nic.in/index1.php?lang=1&level=1&sublinkid=1733&lid=1625 (accessed on 27 Apr 2017). [Google Scholar] |
| 21. | National Family Health Survey 2015-16 (NFHS-4)· District Fact Sheet Madhya Pradesh. Available at www.rchiips.org/nfhs/NFHS-3%20Data/madhya%20pradesh_state_report_for_website_17feb09.pdf (accessed on 6 Apr 2016). [Google Scholar] |
| 22. | Boulet J, Bede C, McKinley D, Norcini J. An overview of the world’s medical schools. Med Teach 2007;29:20-6. [Google Scholar] |
| 23. | Ananthakrishnan N. Medical education in India: Is it still possible to reverse the downhill trend? Natl Med J India 2010;23:156-60. [Google Scholar] |
| 24. | Farmer J, Kenny A, McKinstry C, Huysmans RD. A scoping review of the association between rural medical education and rural practice location. Hum Resour Health 2015;13:27. [Google Scholar] |
| 25. | Rourke J. WHO recommendations to improve retention of rural and remote health workers: Important for all countries. Rural Remote Health 2010;10:1654. [Google Scholar] |
| 26. | Medical Council of India, Establishment of Medical College, Regulations, 1999 (amended up-to March 2016). Available at www.mciindia.org/for-colleges/Estt-of-New-Med-Coll-Regulations-1999.pdf (accessed on 2 Jul 2016). [Google Scholar] |
| 27. | The National Medical Commission Bill; 2016. Available at www.niti.gov.in/writereaddata/files/new_initiatives/MCI%20Bill%20Final.pdf (accessed on 2 Sep 2016). [Google Scholar] |
| 28. | Doctors likely to get 50% quota in PG seats for rural service. The Times of India; 1 January, 2017. Available at www.blogs.timesofindia.indiatimes.com/toi-news/ doctors-likely-to-get-50-quota-in-pg-seats-for-rural-service/ (accessed on 28 Apr 2017). [Google Scholar] |
Fulltext Views
2,710
PDF downloads
9,493



